Stress Urinary Incontinence

The average age of presentation for Stress Urinary Incontinence in Australia is 50-60 years old and commonly occurs after vaginal childbirth. Understandably, leaking urine throughout the day has a hugely detrimental impact on the quality of life for women. The good news is that Stress incontinence management overall has great long term outcomes in regards to no more leakage, high patient satisfaction, quick recovery and low complication rates.
As a certified Urogynaecologist with subspecialty training, Dr Usama Shahid offers expert assessment and management of stress urinary incontinence including complex or recurrent cases. With a focus on holistic care he leads the stress urinary incontinence specialist Wollongong service offering the full range of evidence based treatments, including both mesh and non mesh options. Dr Shahid's focus lies in providing a personalised plan with the goal of achieving durable results and restoring confidence in everyday activities to the women of the Illawarra.

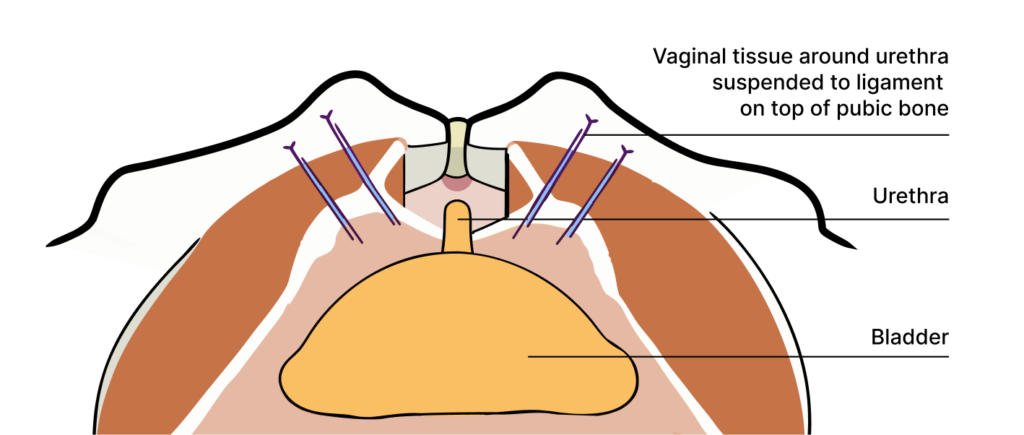
A laparoscopic Burch colposuspension is a minimally invasive surgical treatment for the correction of stress urinary incontinence. There is no mesh used in this procedure.
Under a general anaesthetic, surgical instruments are inserted through small incisions in the abdomen. Following this, the space above the bladder known as the retro-pubic space (or Cave of Retzius) is dissected. The vaginal tissue around the urethra is then elevated, and suspended with permanent sutures to the ileopectineal ligament above the pubic bone. This bladder neck suspension lifts the vagina thus correcting urethral hypermobility by forming a 'hammock' around the urethra to support it. Consequentially, this prevents leakage of urine with increased abdominal pressure from running, coughing, sneezing and jumping.
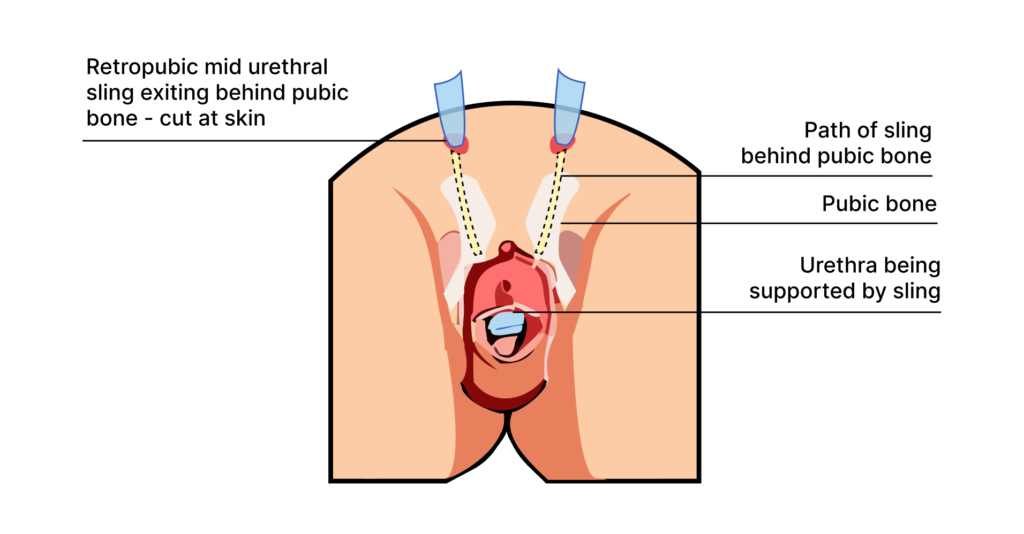
A retropubic mid urethral sling procedure is a minimally invasive surgery used to treat stress urinary incontinence. A narrow permanent strip of synthetic mesh is vaginally placed under the urethra and behind (thus the term 'retro') the pubic bone. This synthetic material forms a sling around the urethra, stabilising it during laughing, coughing, sneezing and running. The procedure has established decades of high success rates, low complications and high patient satisfaction.
Under a general anaesthetic, the bladder is emptied and 2 small incisions are made above the pubic bone. After administering some local anaesthetic to the vagina, an incision is made over the urethra through which the permanent synthetic mesh tape is passed in front of the urethra and exiting behind the pubic bone. A camera is then placed in the bladder to ensure that it was not inadvertently damaged during the procedure. The vaginal incision and exit points behind the pubic bone are then closed with absorbable sutures. If needed vaginal prolapse repairs can be done at the same time as well.
Leaking with laughing, coughing, sneezing or exercise is common, but it is not normal and you don't have to put up with it. With highly subspecialised Urogynaecology training in stress urinary incontinence, Dr Shahid brings to the Illawarra the regions first full time Urogynaecology service.
Through experience in high volume centres, publications of world renowned research and a broad clinical and surgical expertise, Dr Shahid brings a comprehensive and holistic approach in the community he calls home, centring his up to date practice around their care. With an ever growing population in the Illawarra and an increased awareness of stress urinary incontinence, Dr Shahid hopes to restore a sense of normality and confidence to the women he treats.
You don't have to live with leakage.


