Pelvic Organ Prolapse


As a certified Urogynaecologist with subspecialty training, Dr Usama Shahid leads the pelvic organ prolapse specialist Wollongong service providing dedicated expertise in prolapse and an individualised approach to diagnosis and treatment. His subspecialty focus facilitates for a full spectrum of management options from conservative strategies all the way through to advanced pelvic floor reconstructions tailored to your anatomy, symptoms and personal goals. With an overarching goal of restoring function to help you reclaim your life, these comprehensive services are available right now, here in the Illawarra.

Vaginal prolapse is often complex with involvement of multiple compartments that rarely prolapse in isolation but more commonly present together. For this reason, often a time multiple procedures may need to be undertaken at the time of your surgery in order to correct your prolapse.
Below are some surgical procedures which support the upper compartment of vaginal or uterine prolapse.

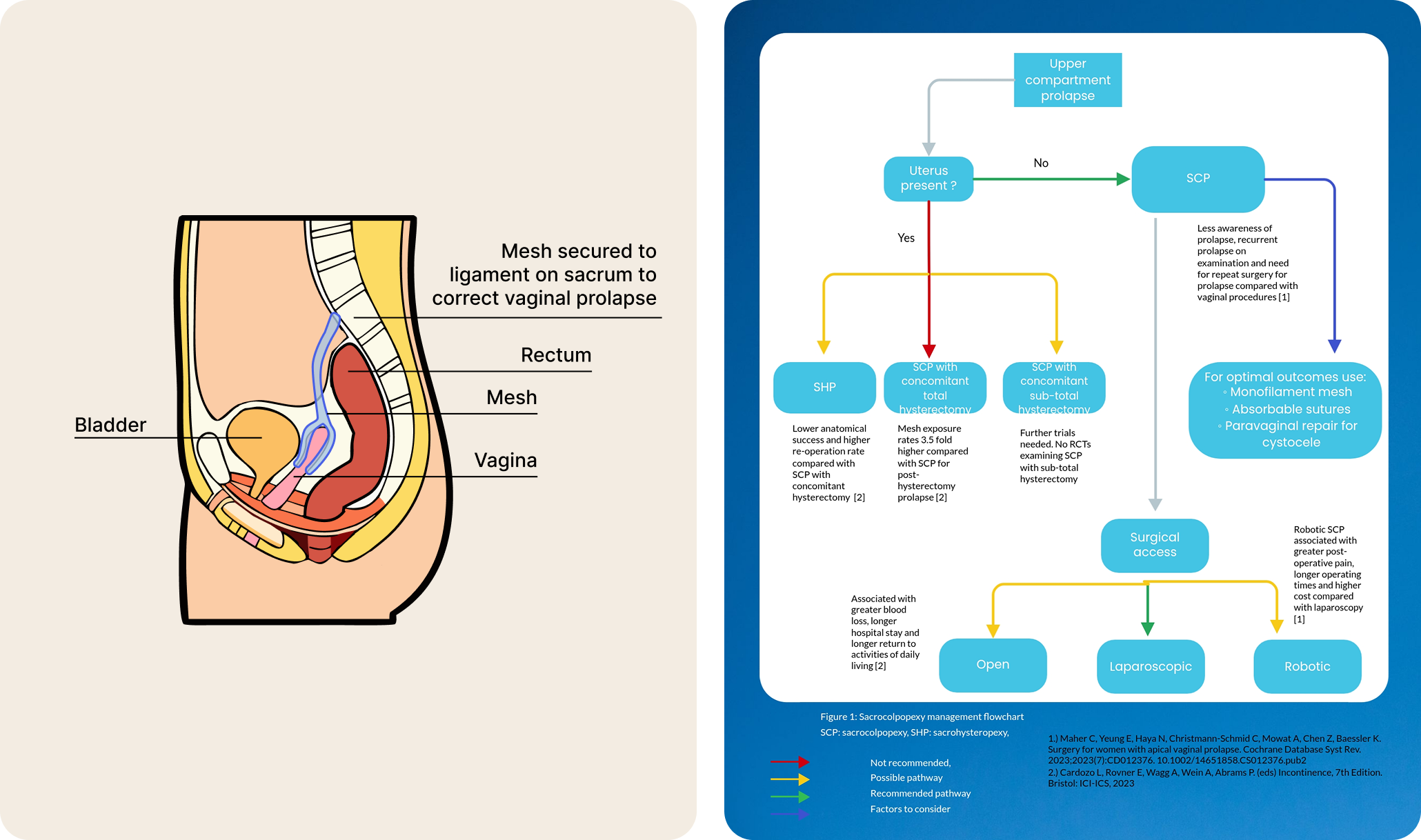
Sacrocolpopexy is a key-hole or minimally invasive procedure which is considered the 'gold-standard' for the surgical correction of vaginal vault prolapse. This is based on good long term outcomes, high patient satisfaction and low complication rates.
Vaginal vault prolapse occurs in people who have had a hysterectomy, causing the top of the vagina to lose its support and drop. Sacrocolpopexy lifts the vagina back to its normal position by suspending it with permanent mesh to a ligament on the sacrum. After dissection of the bladder and rectum, the mesh supports the vagina and the lining of the abdominal cavity (peritoneum) is closed over the mesh. The procedure is often performed concurrently with a paravaginal repair and if needed a posterior repair at the same surgery.
The use of abdominal mesh is very different to that of vaginal mesh (which is no longer used for prolapse in Australia following the Senate enquiry). Due to its location and axis of placement, abdominal mesh has significantly lower rates of mesh related complications compared to vaginal mesh. It is important to understand, that the mesh used for sacrocolpopexy is primarily used for hernia repairs. While this use is considered 'off-label' use, pelvic organ prolapse is a type of hernia. In addition, the mesh has been used abdominally for decades with good outcomes and low rates of complications. Dr Shahid is a subspecialist Urogynaecologist with a refined technique and surgical skillset.
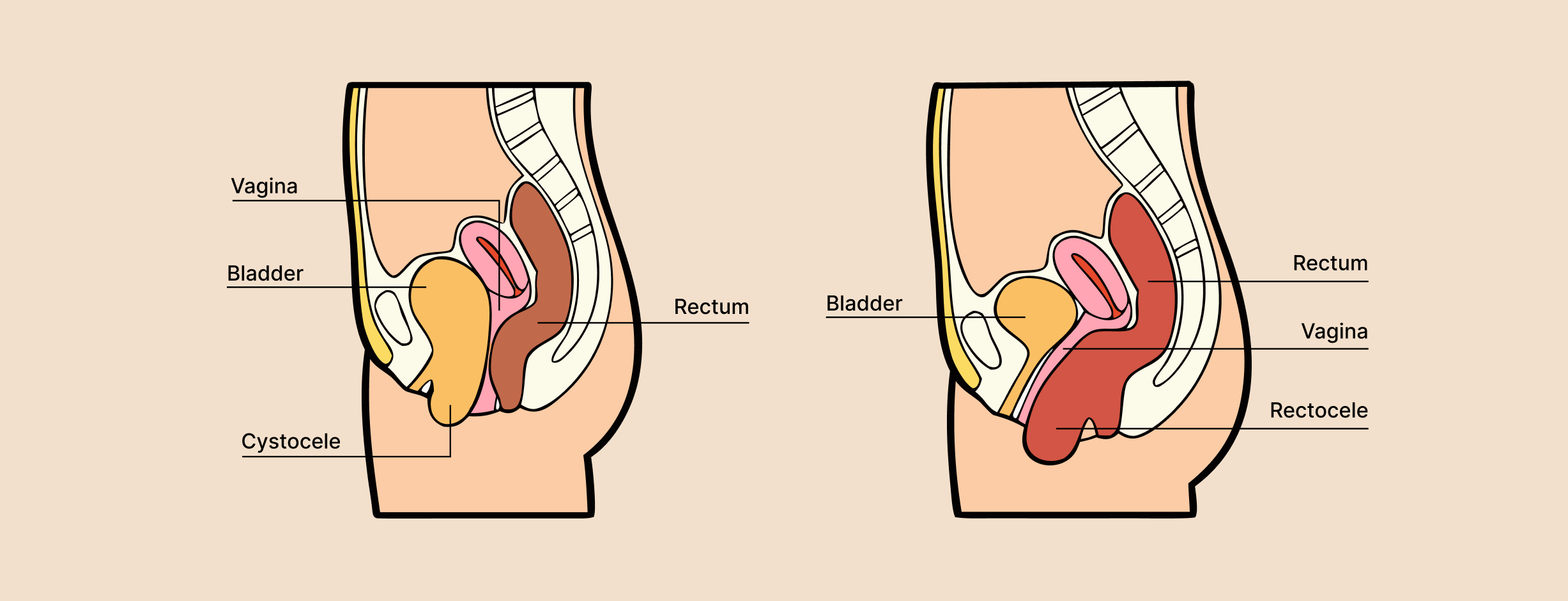
Prolapse of the middle compartment involves the 'front wall' (known as a cystocele) and/or the 'back wall' (known as a rectocele). A cystocele is a type of anterior prolapse that most often involves the bladder while a rectocele is a type of posterior prolapse that involves the rectum. These occur when the bladder and bowel protrudes into the vagina.
Patients may experience bulge symptoms, a difficulty emptying their bowel and/or bladder, sexual dysfunction, urinary tract infections and general discomfort. In some cases, women describe 'manual digitation' whereby they have to insert their fingers into their vagina in order to replace their prolapse and help empty their bowel and/or bladder.
In addition to the conservative (non surgical treatments) mentioned prior, below are a list of the surgical treatment options available for middle compartment prolapse.
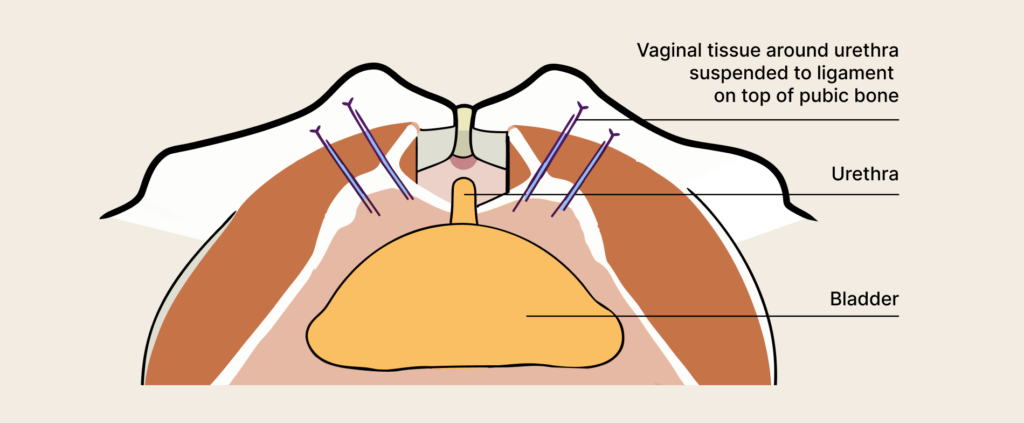
A laparoscopic paravaginal repair is a keyhole operation for the correction of a 'front wall' prolapse otherwise known as a cystocele. The procedure also corrects stress urinary incontinence.
Under a general anaesthetic, surgical instruments are inserted through small incisions in the abdomen. Following this, the space above the bladder known as the retro-pubic space (or Cave of Retzius) is dissected. The vaginal tissue around the urethra is then elevated, and suspended with permanent sutures to the ileopectineal ligament above the pubic bone. This lifts the vagina thus correcting the prolapse and forms a 'hammock' around the urethra thus supporting it.
Prolapse of the lower compartment usually occurs following vaginal childbirth. It is characterised by vaginal laxity or 'looseness' and associated sexual dysfunction through a wide or enlarged genital hiatus. Patients may also complain of vaginal 'flatus' which understandably causes significant embarrassment and distress. Futhermore, since the urethra is also in the lower third of the vagina, patients may also experience stress urinary incontinence which is discussed separately.
In addition to the conservative (non surgical treatments) mentioned prior, a perineoplasty can be considered as part of surgical management for lower compartment prolapse.

Dr Shahid is a Urogynaecologist with a subspecialist focus on pelvic organ prolapse. Through experience in high volume centres, publications of world renowned research and a broad clinical and surgical expertise, he brings to the Illawarra the regions first full time Urogynaecology service.
This allows for a holistic approach to local patients in the community he calls home, centring his up to date practice around their care. With an ever growing population in the Illawarra and an increased awareness of pelvic organ prolapse, Dr Shahid hopes to restore a sense of normality and confidence to the women he treats.


