Recurrent urinary tract infections


rUTIs are defined as having 2 or more urinary tract infections over a 6 month period or more than 3 infections over 12 months. These infections have to be diagnosed with a urine culture test showing bacteria and be associated with symptoms in the absence of an obvious cause (like pregnancy). UTI symptoms include pain with urination, blood in the urine, increased frequency, fever, foul smelling or dark coloured urine and general fatigue.
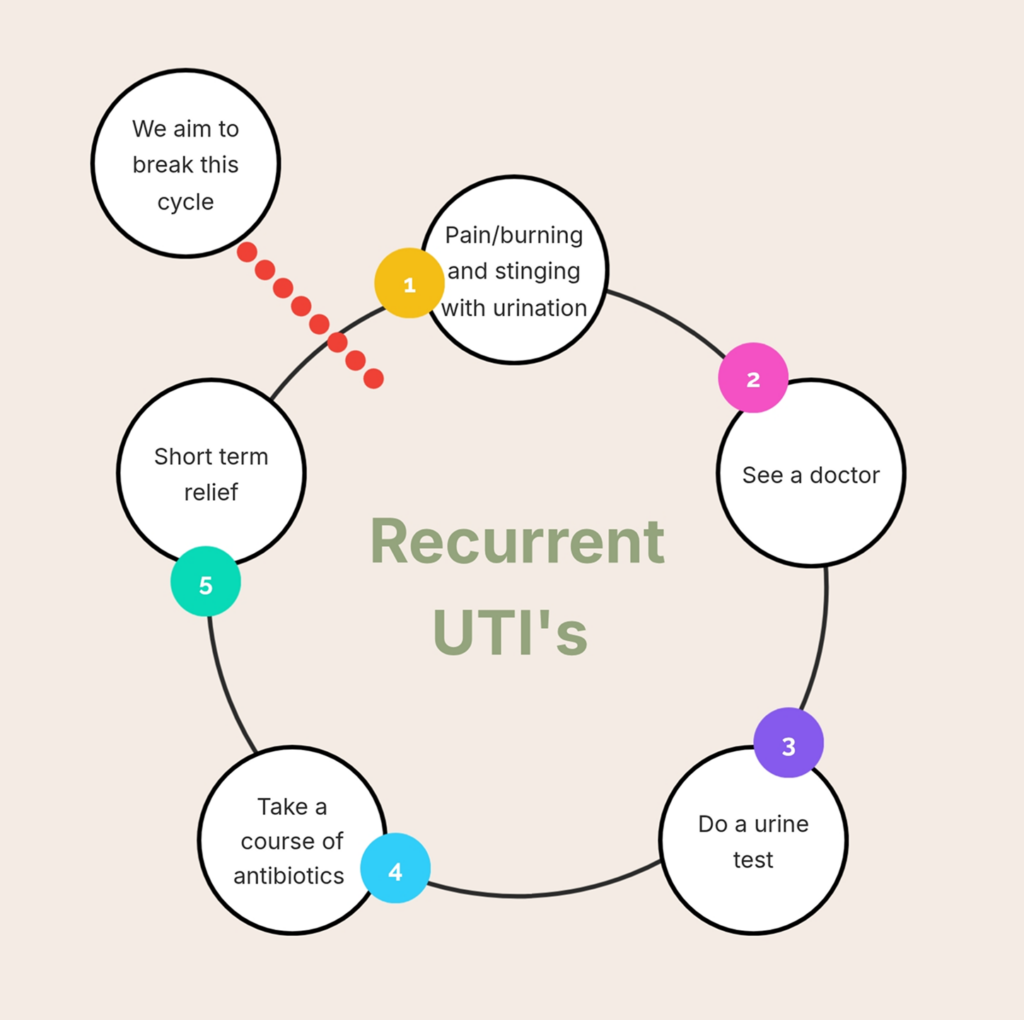
Women with rUTIs tend to be trapped in a cycle of pain, infections, repeated urine tests followed by courses of antibiotics which provide temporary relief before the whole cycle kicks off again. This can be a frustrating and debilitating ordeal which doesn't seem to end.
Recurrent UTI's are not simply bad luck. They are a recognised medical condition with identifiable risk factors and a range of effective management strategies that go well beyond short-term antibiotic treatment. Dr Shahid provides a holistic subspecialist level assessment and a tailored prevention plan to reduce the frequency and severity of your symptoms with the aim of prevent UTIs all together.

Understanding why some women get urinary tract infections (UTIs) is a fundamental step towards developing an individualised management plan and breaking the cycle of recurrent UTIs.
Most cases of UTIs are caused by bacteria known as Escherichia coli (E coli). These bacteria or 'germs' naturally colonise the anus and frequently ascend to the bladder via the urethra when UTIs occur.
A number of factors can increase the risk of rUTIs and need individual treatment for effective UTI prevention:
Recurrent UTI's can be exhausting, distressing and disruptive to your day to day life. They are not something you simply have to live with. There are solutions to this endless cycle of pain, tests and antibiotics.
If you are searching for help with recurrent UTIs, Wollongong-based urogynaecologist Dr Usama Shahid offers comprehensive specialist assessment and personalised prevention strategies right here in the Illawarra.


